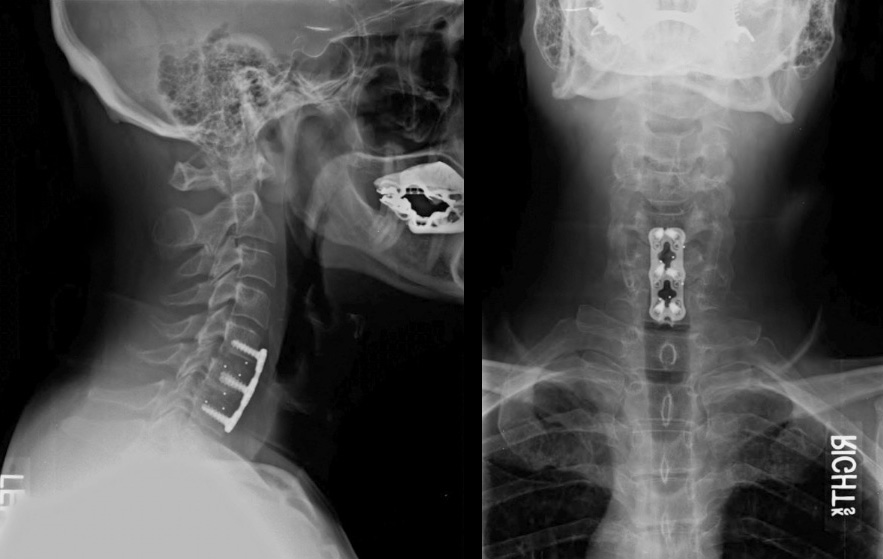
View of the plates
What is ACDF?
Anterior cervical discectomy and fusion (ACDF) is a surgical procedure to treat nerve root or spinal cord compression by decompressing the spinal cord and nerve roots of the cervical spine (neck) with a discectomy and to stabilize the corresponding vertebrae. This procedure is used when other non-surgical treatments have failed.
Typical Symptoms
The typical clinical presentation would be a person who developed acutely or gradually shoulder /arm / hand /finger pain. Additional symptoms can be pins & needles (paraesthesia), numbness or even weakness of involved muscles (eg. grip weakness). A degree of pain or dyscomfort in the neck is also quite common. In a case of severe spinal cord compression gait disturbance (imbalance) or bladder / bowel malfunction as well as limb spasticity can occur ( known as myelopathy).
Details about the Surgery.
Under general anaesthetic the neck is positioned in mild extension. Through a small incision in front (= anterior) of the neck the soft tissue (including oesophagus and trachea) are mobilised to reach the spine. With x-ray the correct disc level is identified. The disc is than completely removed, as well as arthritic bone spurs (osteophytes). This leads to a decompression of the spinal cord and nerve roots. The intervertebral foramen, the bone channel through which the spinal nerve runs, is then enlarged with a drill giving the nerve more room to exit the spinal canal.
To prevent the vertebrae from collapsing and to increase stability, the open space is often filled with bone graft placed inside a spacer (cage) between the vertebral bodies. The slow process of the bone graft joining the vertebrae together is called “fusion”. A titanium plate is screwed on the vertebrae or screws are used between the vertebrae to increase stability during fusion, especially when there is more than one disc involved. A final x-ray is taken on the operating table to ensure correct position of all implants and the alignment of the spine.
Postoperative recovery
The surgery requires a short stay in Hospital (2 to 3 days) and a gradual recovery between 3 to 6 weeks. The patient may be advised to wear a neck brace or collar (for up to 6 weeks), that serves to ensure proper spinal alignment and support. Wearing the brace heightens one’s awareness of posture and positioning and helps prevent movements (e.g., sudden and/or excessive bending or twisting of the neck) that may aggravate or slow down the healing process. In addition, physical therapy and related healing modalities (e.g., massage, acupuncture) may be recommended in order to promote proper healing, as well as to strengthen the surrounding muscles that can take over the neck brace’s job when the patient starts to wean off the neck brace.
It is not unusual in the early phase post surgery to have some wound pain, residual neck pain, some difficulties to swallow or a slightly hoarse voice. All these typically settle within the first 2-4 weeks.